A Holistic Approach To Integrated Care
Our dedicated team of clinicians work together to provide quality behavioral services, helping those in our care to live more positive, active, and social lives.

At School

In-Home

Clinic-Based
Our dedicated team of clinicians work together to provide quality behavioral services, helping those in our care to live more positive, active, and social lives.
SpringHealth Offers Treatment For Children and Adults Diagnosed With:
- Anxiety
- Attention Deficit-Hyperactivity Disorder
- Autism Spectrum Disorder
- Behavioral Disorders
- Depression
- Intellectual Disabilities
What
We Do


We believe in a holistic approach with treating mind and body together. Our evidence-based programming helps SpringHealth deliver the best quality support for our clients to live more positive, active and social lives.
We believe in a holistic approach with treating mind and body together. Our evidence-based programming helps SpringHealth deliver the best quality support for our clients to live more positive, active and social lives.
Individualized Care Settings
SpringHealth offers services and supports in a variety of locations and settings to ensure that the environment where the services are delivered best meet the needs of those in our care.
- Home
- Clinic
- School
- Community
- Telehealth
- Hybrid
Where
We Are
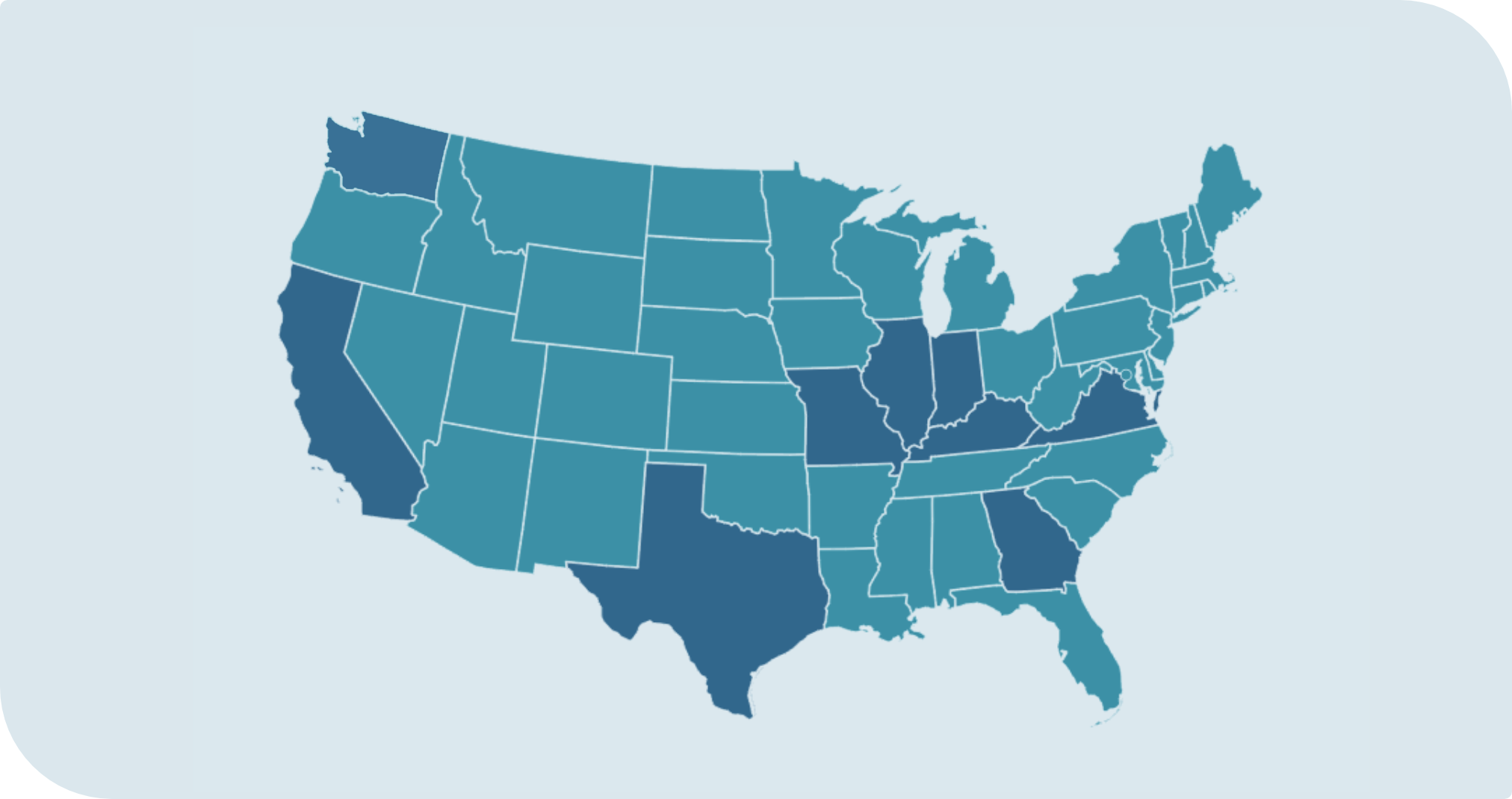
SpringHealth provides behavioral supports and intervention services within multiple states, including California, Georgia, Illinois, Indiana, Kentucky, Missouri, Texas, Virginia and Washington.
SpringHealth provides behavioral supports and intervention services within multiple states, including California, Georgia, Illinois, Indiana, Kentucky, Missouri, Texas, Virginia and Washington.
Join
Our Team

At SpringHealth, our commitment and treatment approach to patient-centered care takes a team effort. We are looking for outstanding individuals to join our team.
At SpringHealth, our commitment and treatment approach to patient-centered care takes a team effort. We are looking for outstanding individuals to join our team.